You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
Since their introduction to dentistry, resin-based composite (RBC) materials have been evolving, by improving in composition, material aspects, condensation techniques, esthetic qualities, technical aspects, polymerization methods, and clinical applications. Good bonding to the tooth structure and adequate polymerization of the resin material are the most important factors for a successful restoration. Clinical efficiency of a light-curing unit is critical for obtaining the optimal polymerization and a successful outcome of RBC restorations.1,2 As discussed in Part I, many modifications have been introduced regarding light-curing units and polymerization techniques and/or methods of RBCs.1,3,4 Part II discusses and highlights the factors that influence the efficiency of light-curing units, as well as the various clinical considerations and precautions for handling and using these units, so as to obtain the maximal efficiency.
Clinical Considerations
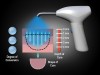
The effectiveness of a light-curing unit to cure efficiently a composite resin material depends on several factors,1,5 such as wavelength of emitted light, type of photoinitiator, bulb intensity, exposure time, distance and angulation of light tip from the composite surface, type of RBC, and shade of the resin composite. Clinical factors influencing the efficiency can be broadly divided into four categories (Figure 1):
- Factors related to RBCs.
- Factors associated with light-curing units.
- Environmental aspects.
- Other issues.
Factors Related to RBCs
Type and Concentration of Fillers and Other Components
A light beam has the maximal intensity near the restoration surface; as it becomes scattered and reflected within the RBC material, it loses intensity. The RBC filler particles tend to scatter the light, and both filler content and size influence the light dispersion.5 Smaller filler particles (0.1 µm to 1.0 µm) have the maximal scattering because these particle sizes correspond to the wavelength range of the photoinitiator. Microfilled composites with smaller or greater particles scatter more light than microhybrids. If the refractive indices of the matrix and filler particles have an increased difference, light scattering is also increased. Therefore, the size and concentration of filler particles should be controlled depending on the refractive indices of the filler and resin matrix, as it influences the color of RBCs.6 Shorter curing times at a given depth or an increased depth of cure for a given exposure time is recommended for overcoming the issue of light scattering by filler particles. The best method is to cure the RBCs in increments of 1.5 mm to 2.0 mm.7 Both the type of curing-light unit used and the RBCs have been shown to interfere with the material’s resistance to abrasion.8 Thus, apart from filler particles, the type of light-curing unit used can influence the material’s wear rate. Also, darker colorants, ultraviolet absorbers, and fluorescent dyes present in RBCs tend to absorb light and can influence the effectiveness of light-curing units.
Shade of RBC Materials
Darker shades and/or more opaque resins tend to absorb more light and thus require longer curing times.5,9 Manufacturers usually specify a recommended curing protocol for individual shade and type of RBCs.
Type of Photoinitiator
A photoinitiator should be present in sufficient concentration so as to react to the proper wavelength of the light-curing unit. An excessive concentration can detrimentally affect the complete curing of RBCs. Most RBCs contain camphorquinone photoinitiators, which can cause an undesirable yellowing of the final esthetics. Thus, whiter and more transparent compounds derived from acylphosphine oxides (eg, monoacylphosphine oxide) and α-diketones (eg, phenylpropanodione [PPD]), also are being used.5 The type of photoinitiator in RBCs significantly influences the curing efficiency of the material across the width of a restoration.10 It also determines the most appropriate light-curing unit to cure a particular type of RBC,5 as the wavelength emitted by a curing unit should match the absorption spectrum or absorption peak of the photoiniator in that RBC. Camphoroquinone-containing RBCs can be readily cured with QTH units and, to a certain extent, by other units.5 The major problem is with PPD- and monoacylphosphine oxide-containing RBCs because most commercially available units either match their spectrum partly or totally fail to do so.5 It is also difficult to cure whiter initiators, such as monoacylphosphine oxide, with LEDs and plasma-arc units (PACs). The wavelength of laser units generally coincides only with the absorption peak of camphoroquinone.11 To overcome this, pairing of these initiators is suggested because it shows a higher conversion rate.12 Thus, for a clinician to appropriately select a light-curing unit for an RBC, the manufacturers should specify on the product labels the required energy output and the spectral bandwidth for the photoinitiated RBCs.13
Factors Associated with Light-Curing Unit
Size of Light-Curing Unit Tip (Tip Geometry)
Light guides are available in diameters of 3 mm, 8 mm, 10 mm, 11 mm, 13 mm, and 14 mm. In a light-curing unit that has a standard diameter tip (11 mm), the light energy is more diffused, whereas in a light-curing unit with a smaller tip (3-mm turboguide), it is more concentrated (Figure 2). These small-diameter tips of light-curing units increase the output of light energy by 8-fold but also raise the temperature of the restoration and tooth structure during curing.14 Therefore, they should be used cautiously. Also, the light intensity from the light-curing unit tip falls off from the center to the edges, forming a bullet-shaped curing pattern (Figure 3). This variability in light intensity across the curing-tip face can cause improper curing of RBCs in proximal box restorations and extensive restorations.10 Recently, it has been suggested to use an R value to describe the light guide shape rather than words such as "normal" or "turbo."15 An R value is the ratio between the entry diameter and exit diameter of the light guide tips. A higher R value tip is more efficient if the tip to composite distance is less than 5 mm. For more than 5 mm, tips with a lower R value are better.15 The R value also influences the curing depths of the RBCs.
Type of Light-Curing Unit
Each light-curing unit has its own wavelength specifications, advantages, disadvantages, and curing efficiency. It has been observed that more light is absorbed by the RBCs with the laser units and scattering is greater with the quartz-tungsten-halogen (QTH) units.16 Due to the broad wavelengths spectra available for QTH units, the decrease in light penetration caused by increased light scattering of shorter wavelengths is compensated by the longer wavelengths, which can easily transmit through the material and reach the deeper layers. Although the lights of laser units have better absorption, the devices have limited bandwidth and emit wavelengths closer to the absorption peak of the photoinitiator. Thus, QTH units are more efficient than laser ones for visible light-cured RBCs. Conversely, due to its inherent property of coherency, there is no loss of power in the distance in laser units as seen in QTH units. Therefore, they are the units of choice for inaccessible areas.5
Exposure Time
Adequate curing of RBCs and dentin bonding agents not only depends on curing-light units but also on the exposure duration or exposure time.7,17 A standard time of 20 secs is usually required to cure to a depth of 2.0 mm to 2.5 mm by most curing-light units having a power density of 800 mW/cm2. For a unit emitting 400 mW/cm2, an exposure time of 40 secs is required to cure through a 2-mm thick layer of an RBC. Thus, increasing the power density of the lamp reduces the required exposure time at a given depth and also increases the rate and degree of cure.2 Also, because the energy density is a product of intensity multiplied by exposure time,18 the same energy can be consumed at high or low intensities by modifying the exposure time to maximize the energy efficiency. An exposure time of 40 secs is considered optimal for all curing-light units used for RBCs.19,20 The required exposure time can be influenced by the type of light-curing unit, shade of RBCs,9 and RBC formulation.21 Thus, a universal exposure time as recommended by the manufacturers cannot be used for all clinical scenarios and operating conditions. It has been observed that exposure times longer than those recommended are required to optimize the flexural strength for an incremental thickness of an RBC.22 To determine the exact exposure durations required to obtain optimal properties of RBCs, a compule-scrape test has been advocated, which is a simple in-office chairside scraping procedure designed to develop a customized exposure guide.22 Compules of RBCs are modified to form cylinders in which their contents are forced to one end and photopolymerized (at a 2-mm distance) for various exposure durations. Compule contents are extruded 24 hours later, and the unpolymerized residue is removed using hand scraping with a plastic spatula. The thickness of the resulting specimen is measured as a function of exposure duration.
Light Source (Lamp Output Intensity)
The lamp intensity is determined by its power rating and light-guide diameter.5 An adequate energy density (ie, intensity multiplied by exposure time) is required for proper curing of RBCs.23 Therefore, lamp output intensity should always be maintained for a longer clinical life of the curing unit. Usually, light output of the lamp and its curing effectiveness reduces with time. This is mainly caused by the alternate heating and cooling of the tip surface, leading to dulling or clouding of the tip due to the condensation of mercury vapors, vapors from bonding system solvents, or moisture. At times, the resin adheres to the tip during curing, scattering the light, and reduces the effectiveness of curing-light unit. Therefore, it is important to routinely clean the mirror surface with cotton swabs dipped in alcohol or methyl ethylketone solvents or by using a rubber wheel on a slow-speed handpiece. This tends to preserve and renew the reflection effectiveness of the bulb.
Angulation of Light Tip
A light beam creates a circular spot of light when held perpendicular to the restoration surface. The wand tip of the curing-light unit should always be parallel to the restoration surface to achieve maximal light intensity at the surface. As the wand is tipped, the circular shape changes to an ellipse (greater surface area) and thus decreases the light intensity as energy is spread over a greater area.24
Beam Spreading
The light beam usually disperses from its origin from the curing-light unit tip, leading to inhomogeneous distribution of light intensity (Figure 3). Thus, as the wand is moved away from the resin surface, both the light intensity and amount of curing decreases. At distances beyond 6 mm for QTH lights, the output may be less than one third that at the tip. This inhomogeneity can result in inhomogeneous polymerization below the light guide tip.25 Therefore, it is necessary to "step" the light across a large restoration so as to adequately cure the entire surface. Also, to permit closer approximation to an RBC restoration, light-transmitting wedges have been promoted for interproximal curing and light-focusing tips to access proximal boxes. A simple test to check for beam spreading is to note the diameter of the light spot. If the diameter that is created by a light beam directed perpendicularly onto a surface from a distance of about 100 mm is the same as the diameter from that of the wand tip, then there is no beam spreading.24 It is also advocated to use an exposure time of 60 secs with larger emitting tips.
Color Changes in RBCs Following Light Curing
RBC materials often show perceptible color changes during polymerization, which are usually unacceptable.26,27 QTH-curing lights tend to demonstrate more yellowing of RBCs than light-emitting diodes (LEDs).28 Thus, for a precise shade match for RBCs, a custom shade guide should be fabricated using cured resin samples. This is employed with a universal shade guide for the shade selection of RBCs.
Distance of Curing Tip From the RBC Surface
The light intensity striking the RBC restoration surface is inversely proportional to the distance from the tip of the fiber optic bundle of the curing light to the composite surface.5 Also, for all light-curing units, the depth of cure generally decreases as the distance from the tip increases.29 Ideally, the tip should be within 3 mm of the RBC to be effective.30 For the darkest shades, increments should be limited to 1 mm of thickness. While both intensity and depth of cure decrease with increasing distance,29,30 the relationship between these factors and distance may not be similar for all curing lights.31
Temperature Rise During Curing
A potential risk of heat-induced pulpal injury has been proposed during light curing of RBCs because the temperature rise during curing can be in excess of the values normally quoted as causing irreversible pulp damage.32 The risk is greater with high-energy as compared with low-energy output systems.33,34 Light intensity and exposure time appear to be the most important factors causing temperature change when curing RBCs.33,35 The mean pulp temperature rise produced by different light-curing units in ascending order is: QTH, LEDs, enhanced halogen curing lights, and PAC units. The major rise in temperature occurs during the curing of the bonding agent as compared with curing of RBCs.35,36 Recent studies have shown that although the light-curing units cause a temperature rise in the pulp chamber, none has exceeded the critical value of 5.5ºC.37,38 Thus, to avoid any thermal damage to the pulp, a correct choice of a light-curing unit and curing time is important when polymerizing light-activated RBCs. Also, the curing of bonding agents should be performed with low-intensity light, and high-intensity should be used only for curing of RBCs regardless of the light-curing unit used.
Effect of Autoclaving on Light-Curing Tips
During autoclaving, boiler scale tends to form on the instruments being sterilized, including the light-curing tip. This can compromise the intensity of irradiation transmitted from the bulb of light-curing units.39 The effect can be minimized by polishing the tip regularly between autoclaving processes.
Degree of Conversion/Degree of Cure
The degree of conversion (DOC) is the percentage of carbon-carbon double bonds that have been converted to single bonds to form a polymeric resin. Bisphenol A diglycidylether methacrylate (bis-GMA)-based RBCs have a DOC of 55% to 65%, which implies 55% to 65% of the methacrylate groups has been polymerized following curing of the material. This is due to the steric hindrance of the reacting molecules. The higher the DOC is, the better the mechanical properties (strength, wear resistance) of the RBCs. It is directly proportional to the light intensity and exposure time and inversely proportional to the depth of cure into an RBC material.30,40 There is no difference between the DOC of chemically activated and light-activated RBCs with the same monomer formulations. Recently, certain high-conversion, high-strength monomer systems have been introduced to reduce the effects of residual unsaturation that may impair the mechanical and chemical properties of RBCs. These include:
- Increasing the content of triethyleneglycol-dimethacrylate (TEGDMA) in a bis-GMA:TEGDMA comonomer. This will increase conversion but will make the material very brittle and fracture prone.
- The use of a more reactive diluent monomer (α-methylene-γ-butyrolactone) has shown to increase the conversion rate without hampering the mechanical properties.41 The degree of crosslinking in the polymer matrix could be increased by the addition of carboxylic anhydrides to develop a mechanically stronger and more wear-resistant RBC.42 Aldehyde and diketone are thought to increase the degree of crosslinking by reacting with methacrylate double bonds and other pendant and backbone functional groups.
Factors Associated with Environment
Effect of Surrounding Atmosphere
The light intensity at the surface of an RBC restoration is inversely proportional to the distance from the tip of the light-curing unit to the RBC surface.5 This is due to the scattering of light by air molecules on the path to the restoration surface. Thus, the tip should be within 3 mm of the RBC’s thickness and for darkest shades within 1 mm of thickness of RBC to effectively cure the restoration.
Effect of Ambient and Operating Light
In single-handed dentistry, usually there are high chances of exposure of RBC material to the ambient and/or the operating light, which can initiate premature curing. This results in difficulty in handling the RBC and reduced working time. The use of yellow filters and polyester-based photographic filters is effective in avoiding this unwanted activation and in extending the working time.43 Employing prepacked compules of RBC material also may help prevent this premature curing of the material.
Other Factors
Effect of Tooth Structure
As the light passes through tooth structure (enamel or dentin), it is absorbed and scattered, resulting in incomplete curing of RBC material, especially in areas such as proximal boxes. This effect depends on the thickness and optical behavior of intervening material.1 Enamel is very transparent and allows the passage of a great deal of light, whereas dentin is considerably less transparent and allows virtually no light to penetrate. Thus, the exposure time has to be increased by a factor of 2 to 3 when attempting to polymerize the restoration through the tooth structure.44
Conclusion
Apart from the type of light-curing unit employed, the clinician’s knowledge and clinical skill in handling and maneuvering these units play a decisive role in the polymerization and final outcome of RBC restorations. Many factors associated with RBCs, light-curing units, and surrounding environment can influence the polymerization kinetics of RBCs and clinical effectiveness of curing units. Clinical tips that may help in proper curing of RBCs are as follows:
- Select a light-curing unit, taking into consideration the composition (photoinitiator and fillers) and shade of RBCs.
- Cure the RBCs in 2-mm increments, using a light-curing tip of appropriate R value.
- Cure the restoration for at least 40 secs from a distance of 1 mm to 3 mm, keeping the unit tip perpendicular to the restoration surface.
- "Step" the light-curing unit across a large restoration.
- Use yellow or polyester-based photographic filters to extend the working time.
- Increase the exposure time to two to three times when curing through the tooth structure. Use light-transmitting wedges and focusing tips during curing of proximal restorations.
- Use a custom shade guide fabricated from cured resins, as well as a universal shade guide for shade selection.
- Routinely clean the mirror surface and polish the unit tips to preserve the reflection effectiveness of the light-curing unit.
- Choose low-intensity light-curing units for curing of bonding agents.
- Regularly check the output intensity, energy density, and beam spreading of a light-curing unit.
References
1. Jiménez-Planas A, Martin J, Abalos C, et al. Developments in polymerization lamps. Quintessence Int. 2008;39(2):e74-e84.
2. Resin composite restorative materials. In: Powers JM, Sakaguchi RL, eds. Craig’s Restorative Dental Materials. 12th ed. St. Louis, MO: Mosby; 2007:189-182.
3. Rawls RH, Esquivel-Upshaw JF. Restorative resins. In: Anusavice KJ, ed. Philip’s Science of Dental Materials. 11th ed. St. Louis, MO: Mosby; 2003:399-442.
4. Wakefield CW, Kofford KR. Advances in restorative materials. Dent Clin North Am. 2001;45(1):7-29.
5. Bayne SC, Thompson JY, Taylor DF. Dental materials. In: Roberson TM, Heymann HO, Ritter AV, eds. Sturdevant’s Art and Science of Operative Dentistry. 4th ed. St. Louis, MO: Mosby; 2002:134-234.
6. Lee YK. Influence of scattering/absorption characteristics on the color of resin composites. Dent Mater. 2007;23(1):124-131.
7. Ceballos L, Fuentes MV, Tafalla H, et al. Curing effectiveness of resin composites at different exposure times using LED and halogen units. Med Oral Patol Oral Cir Bucal. 2009;14(1):e51-e56.
8. Martinelli J, Pires-de-Souza Fde C, Casemiro L A, et al. Abrasion resistance of composites polymerized by light-emitting diodes (LED) and halogen light-curing units. Braz Dent J. 2006;17(1):29-33.
9. Hilton TJ. Direct posterior esthetic restorations. In: Summit JB, Robbins JW, Schwartz RS, eds. Fundamentals of Operative Dentistry. Chicago, IL: Quintessence; 2001:260-305.
10. Palin WM, Senyilmaz DP, Marquis PM, et al. Cure width potential for MOD resin composite molar restorations. Dent Mater. 2008;24(8):1083-1094.
11. Meniga A, Tarle Z, Ristic M, et al. Pulsed blue laser curing of hybrid composite resins. Biomaterials. 1997;18(20):1349-1354.
12. Park YJ, Chae KH, Rawls HR. Development of new photoinitiation system for dental light-cure composite resins. Dent Mater. 1999;15(2):120-127.
13. Suh BI. Controlling and understanding the polymerization shrinkage-induced stresses in light-cured composites. Compend Contin Educ Dent. 1999;25(suppl):S34-S41.
14. Loney RW, Price RB, Temperature transmission of high-output light-curing units through dentin. Oper Dent. 2001;26(5):516-520.
15. Corciolani G, Vichi A, Davidson CL, et al. The influence of tip geometry and distance on light-curing efficacy. Oper Dent. 2008;33 (3):325-331.
16. Emami N, Sjödahl M, Söderholm KJ. How filler properties, filler fraction, sample thickness and light source affect light attenuation in particulate filled resin composites. Dent Mater. 2005;21(8):721-730.
17. Ye Q, Wang Y, Williams K, et al. Characterization of photopolymerization of dentin adhesives as a function of light source and irradiance. J Biomed Mater Res B Appl Biomater. 2007;80(2):440-446.
18. Abate PF, Zahra VN, Macchi RL. Effect of photopolymerization variables on composite hardness. J Prosthet Dent. 2001;86(6):632-635.
19. Antonson SA, Antonson DE, Hardigan PC. Should my new curing light be an LED? Oper Dent. 2008;33(4):400-407.
20. David JR, Gomes OM, Gomes JC, et al. Effect of exposure time on curing efficiency of polymerizing units equipped with light-emitting diodes. J Oral Sci. 2007;49(1):19-24.
21. Cavalcante LM, Valentino TA, Carlini B Jr, et al. Influence of different exposure time required to stabilize hardness values of composite resin restorations. J Contemp Dent Pract. 2009;10(2):42-50.
22. Rueggeberg FA, Cole MA, Looney SW, et al. Comparison of manufacturer-recommended exposure durations with those determined using biaxial flexure strength and scraped composite thickness among a variety of light-curing units. J Esthet Restor Dent. 2009;21(1):43-61.
23. Gritsch K, Souvannasot S, Schembri C, et al. Influence of light energy and power density on the microhardness of two nanohybrid composites. Eur J Oral Sci. 2008;116(1):77-82.
24. Williams PT, Johnson LN. Composite resin restoratives revisited. J Can Dent Assoc. 1993;59(6):538-543.
25. Arikawa H, Kanie T, Fujii K, et al. Effect of inhomogeneity of light from light curing units on the surface hardness of composite resin. Dent Mater J. 2008;27(1):21-28.
26. Sidhu S K, Ikeda T, Omata Y, et al. Change of color and translucency by light curing in resin composites. Oper Dent. 2006;31(5):598-603.
27. Tak O, Altintas S H, Ozturk N, et al. Effect of three types of light-curing units on 5-year colour changes of light-cured composite. Clin Oral Investig. 2009;13(1):29-35.
28. Brackett MG, Brackett WW, Browning WD, et al The effect of light curing source on the residual yellowing of resin composites. Oper Dent. 2007;32(5):443-450.
29. Dunne SM, Millar BJ. Effect of distance from curing light tip to restoration surface on depth of cure of composite resin. Prim Dent Care. 2008;15(4):147-152.
30. Rode KM, de Freitas PM, Lloret PR, et al. Micro-hardness evaluation of a micro-hybrid composite resin light cured with halogen light, light-emitting diode and argon ion laser. Lasers Med Sci. 2009;24(1):87-92.
31. Aravamudhan K, Rakowski D, Fan PL. Variation of depth of cure and intensity with distance using LED curing lights. Dent Mater. 2006;22(11):988-994.
32. Bagis B, Bagis Y, Ertas E, et al. Comparison of the heat generation of light curing units. J Contemp Dent Pract. 2008;9(2):65-72.
33. Guiraldo RD, Consani S, Lympius T, et al. Influence of the light curing unit and thickness of residual dentin on generation of heat during composite photoactivation. J Oral Sci. 2008;50(2):137-142.
34. Yazici A R, Müftü A, Kugel G. Temperature rise produced by different light-curing units through dentin. J Contemp Dent Pract. 2007;8(7):21-28.
35. Durey K, Santini A, Miletic V. Pulp chamber temperature rise during curing of resin-based composites with different light-curing units. Prim Dent Care. 2008;15(1):33-38.
36. Millen C, Ormond M, Richardson G, et al. A study of temperature rise in the pulp chamber during composite polymerization with different light-curing units. J Contemp Dent Pract. 2007;8(7):29-37.
37. Yazici AR, Müftü, Kugel G, et al. Comparison of temperature changes in the pulp chamber induced by various light curing units, in vitro. Oper Dent. 2006;31(2):261-265.
38. Hubbezoglu I, Dogan A, Dogan OM, et al. Effects of light curing modes and resin composites on temperature rise under human dentin: in vitro study. Dent Mater J. 2008;27(4):581-589.
39. Rueggeberg FA, Caughman WF, Comer RW. The effect of autoclaving on energy transmission through light-curing tips. J Am Dent Assoc. 1996;127(8):1183-1187.
40. Atmadja G, Bryant RW. Some factors influencing the depth of cure of visible light-activated composite resins. Aust Dent J. 1990;35(3):213-218.
41. Stansbury JW, Antonucci JM. Evaluation of methylene lactone monomers in dental resins. Dent Mater. 1992;8(4):270-273.
42. Peutzfeldt A, Asmussen E. Influence of carboxylic anhydrides on selected mechanical properties of heat-cured resin composites. J Dent Res. 1991;70(12):1537-1541.
43. Jacobsen PH. Extending the working time of light-activated composite restorative materials. Br Dent J. 1986;160(5):162-165.
44. Belvedere PC. Contemporary posterior direct composites using state-of-the-art techniques. Dent Clin North Am. 2001;45(1):49-70.
About the Authors
Neeraj Malhotra, MDS, Assistant Professor, Department of Conservative Dentistry and Endodontics, Manipal College of Dental Sciences, Mangalore, India
Kundabala Mala, MDS, Professor, Department of Conservative Dentistry and Endodontics, Manipal College of Dental Sciences, Mangalore, India